Hook plate στην κλείδα & AC dislocations: αποτελεσματική, αλλά όχι “αθώα”.
Η hook plate στα περιφερικά κατάγματα της κλείδας και στα κατάγματα-εξαρθρήματα / AC dislocations είναι μια αποτελεσματική αλλά όχι “αθώα” λύση. Κατά τη γνώμη μου, παραμένει χρήσιμο εργαλείο σε επιλεγμένες περιπτώσεις, αλλά δεν είναι πλέον η ιδανική πρώτη επιλογή για όλους.
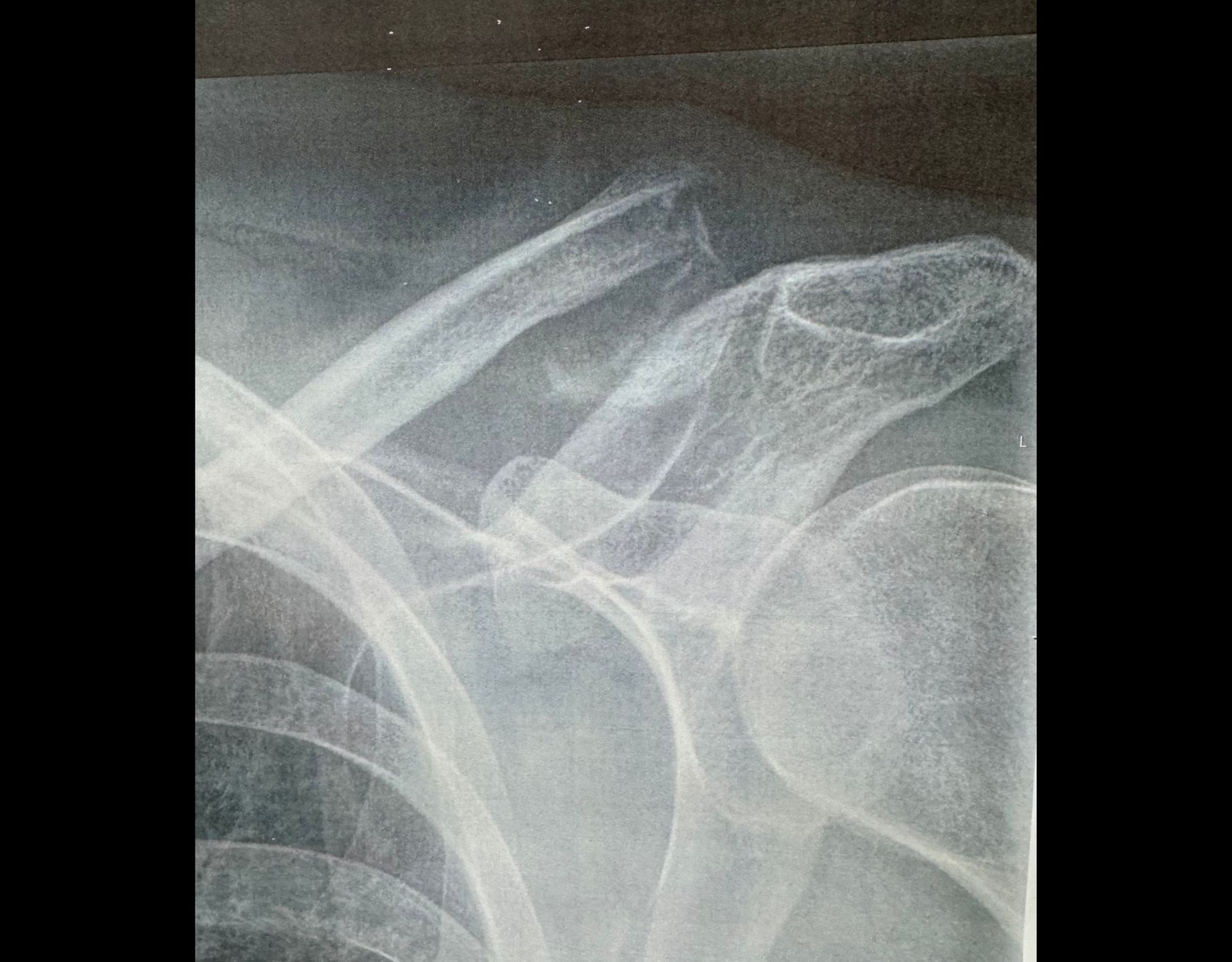
Στα ασταθή περιφερικά κατάγματα της κλείδας, ιδίως όταν το περιφερικό τεμάχιο είναι μικρό, πολυτεμαχισμένο ή δεν “κρατάει” καλά βίδες, η hook plate έχει το πλεονέκτημα ότι δίνει έμμεση σταθεροποίηση και συχνά επιτρέπει αξιόπιστη πώρωση χωρίς να χρειάζεται μεγάλη αγορά οστού στο έξω τμήμα. Αυτός είναι και ο βασικός λόγος που εξακολουθεί να χρησιμοποιείται.
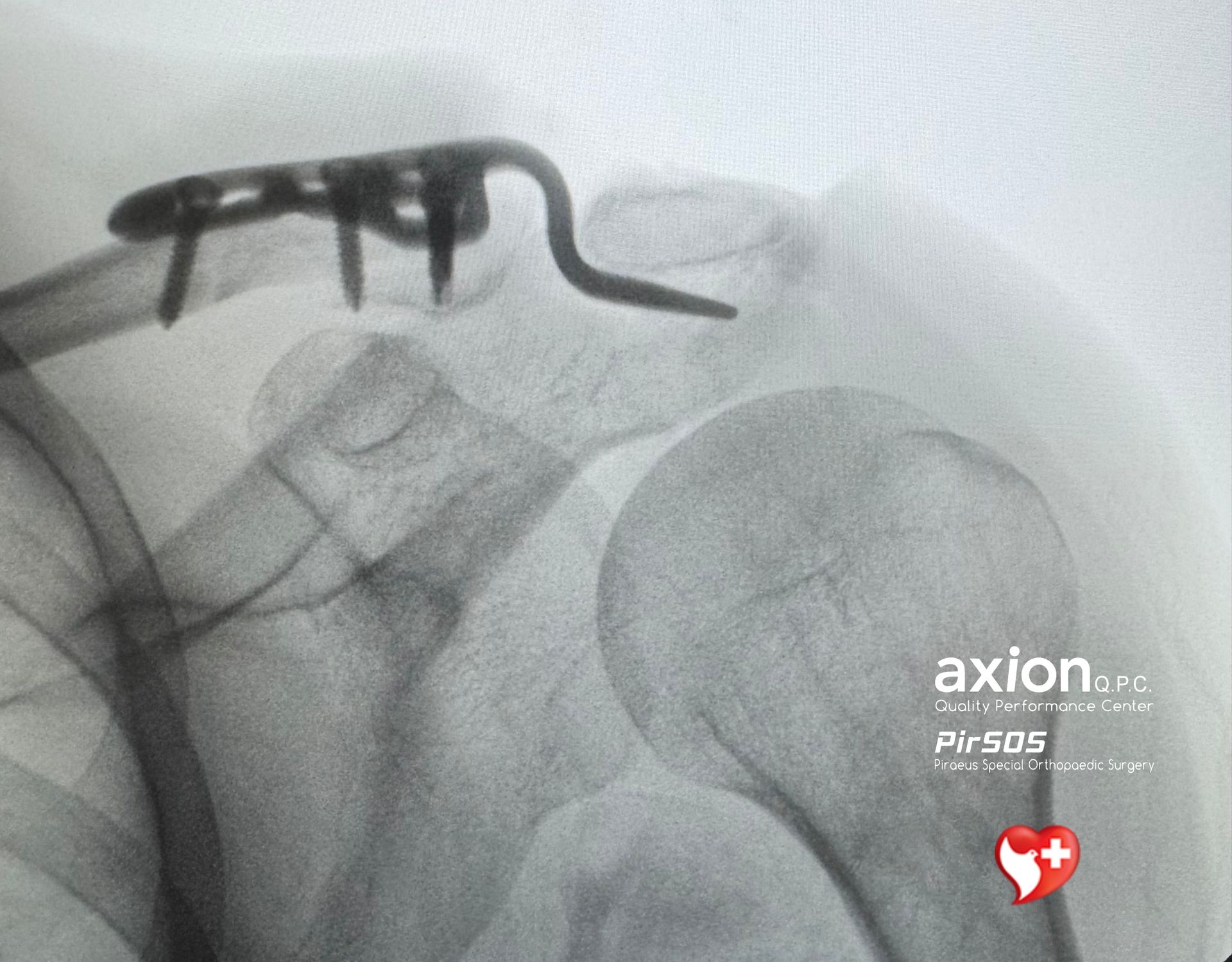
Όμως το κύριο πρόβλημα είναι ότι η hook plate δουλεύει υποακρωμιακά, άρα η ίδια η μηχανική της σχετίζεται με επιπλοκές όπως: subacromial impingement , erosion/osteolysis του ακρωμίου, άλγος, δυσκαμψία, περιορισμό ώμου, και όχι σπάνια την ανάγκη δεύτερου χειρουργείου για αφαίρεση του υλικού.
Ειδικά για τα Neer type II lateral clavicle fractures, οι πιο σύγχρονες συγκριτικές αναλύσεις και η AAOS guideline αναφέρουν ότι οι lateral locking plates έχουν συνήθως λιγότερες επιπλοκές και καλύτερα λειτουργικά αποτελέσματα από τις hook plates, όταν φυσικά η ανατομία του κατάγματος επιτρέπει τη χρήση τους.
Στα AC joint dislocations , η hook plate επίσης μπορεί να δώσει πολύ καλή ανάταξη, αλλά και εκεί οι νεότερες μετα-αναλύσεις δείχνουν ότι τεχνικές coracoclavicular suspension/reconstruction συχνά έχουν λιγότερες επιπλοκές και αποφεύγουν ευκολότερα το θέμα της υποχρεωτικής αφαίρεσης.
Συμπέρασμα: Η hook plate δεν είναι κακή μέθοδος· είναι αποτελεσματική, αλλά μάλλον salvage / selective indication method παρά η ιδανική ρουτίνα για κάθε περιφερικό κάταγμα ή εξάρθρημα κλείδας.
Ναι όταν το distal fragment είναι δύσκολο και δεν επιτρέπει καλύτερη λύση. Όχι ως πρώτη σκέψη όταν μπορείς να κάνεις σταθερή οστεοσύνθεση με locking plate και συμπληρωματική CC σταθεροποίηση.
The use of a hook plate in distal clavicle fractures and fracture–dislocations / AC joint dislocations is an effective but not entirely “innocent” solution. In my opinion, it remains a valuable tool in selected cases, but it is no longer the ideal first-line option for all patients.
In unstable distal clavicle fractures—particularly when the distal fragment is small, comminuted, or does not allow secure screw fixation—the hook plate offers the advantage of indirect stabilization and often enables reliable healing without substantial bone purchase in the lateral fragment.
However, due to its subacromial position, hook plates are inherently associated with complications such as subacromial impingement , acromial erosion/osteolysis , pain, stiffness, limitation of shoulder motion, and not infrequently the need for a second procedure for implant removal.
For Neer type II distal clavicle fractures, recent comparative studies and AAOS guidance suggest that lateral locking plates are generally associated with fewer complications and better functional outcomes than hook plates, provided the fracture anatomy allows their application.
In AC joint dislocations , hook plates can achieve excellent reduction, but recent meta-analyses suggest that coracoclavicular suspension/reconstruction techniques often have fewer complications and more easily avoid mandatory implant removal.
Conclusion: Hook plates are effective, but best considered a selective/salvage option rather than a routine first-line solution when stable fixation can be achieved with a distal locking plate and CC augmentation.
Selective indication over routine use.
Die Verwendung einer Hook-Plate bei distalen Klavikulafrakturen und AC-Gelenkverletzungen ist wirksam, aber nicht völlig „harmlos“. Meiner Meinung nach bleibt sie in ausgewählten Fällen ein nützliches Instrument, ist jedoch nicht mehr die ideale Erstlinienoption für alle Patient:innen.
Insbesondere bei instabilen distalen Klavikulafrakturen mit kleinem oder mehrfragmentärem distalem Fragment kann die Hook-Plate eine indirekte Stabilisierung ermöglichen und eine zuverlässige knöcherne Heilung unterstützen.
Der wesentliche Nachteil liegt in der subakromialen Lage: Komplikationen wie subakromiales Impingement , Erosion/Osteolyse des Akromions, Schmerzen, Steifigkeit und Bewegungseinschränkung sind möglich; nicht selten ist eine Materialentfernung erforderlich.
Bei Neer Typ II -Frakturen zeigen aktuelle Vergleiche und Empfehlungen, dass distale Locking-Plates (sofern anatomisch möglich) häufig mit weniger Komplikationen und besseren funktionellen Ergebnissen verbunden sind.
Auch bei AC-Gelenkluxationen kann die Hook-Plate eine sehr gute Reposition erzielen. Neuere Meta-Analysen zeigen jedoch, dass Verfahren der korakoklavikulären Suspension/Rekonstruktion häufig mit weniger Komplikationen verbunden sind und die „obligate“ Materialentfernung eher vermeiden.
Fazit: Die Hook-Plate ist nicht „schlecht“ – sie ist wirksam, sollte jedoch eher als selektive/salvage Option betrachtet werden und nicht als Routine-Erstlinienverfahren, wenn eine stabile Fixation mit distaler Locking-Plate und CC-Augmentation möglich ist.
Selektive Indikation statt Routine.
El uso de una hook plate en fracturas distales de clavícula y luxaciones / lesiones de la articulación acromioclavicular (AC) es una solución eficaz, pero no completamente “inocente”. En mi opinión, sigue siendo una herramienta valiosa en casos seleccionados, pero ya no es la opción ideal de primera línea para todos los pacientes.
En fracturas distales inestables —especialmente cuando el fragmento distal es pequeño, conminuto o no permite una fijación segura con tornillos— la hook plate ofrece la ventaja de una estabilización indirecta y con frecuencia permite una consolidación fiable sin requerir una gran compra ósea en el fragmento lateral.
Sin embargo, su principal desventaja es su posición subacromial. Su mecánica se asocia con complicaciones como impingement subacromial , erosión/osteólisis del acromion, dolor, rigidez y limitación del movimiento del hombro. No es infrecuente la necesidad de una segunda cirugía para retirar el implante.
En fracturas laterales de clavícula Neer tipo II , estudios comparativos recientes y recomendaciones indican que las placas bloqueadas laterales suelen asociarse con menos complicaciones y mejores resultados funcionales que las hook plates, siempre que la anatomía de la fractura lo permita.
En luxaciones de la articulación AC , la hook plate también puede lograr una excelente reducción, pero meta-análisis más recientes sugieren que técnicas de suspensión/reconstrucción coracoclavicular a menudo presentan menos complicaciones y evitan más fácilmente la necesidad de una retirada obligatoria del implante.
Conclusión: La hook plate no es un mal método; es eficaz, pero debería considerarse más como una opción selectiva/salvamento que como una técnica rutinaria de primera línea cuando puede lograrse una fijación estable con una placa bloqueada distal y aumento CC.
Indicación selectiva, no rutina.